
From the 1Department of Rehabilitation Medicine, and Australian Rehabilitation Research Centre, Royal Melbourne Hospital, Parkville, Victoria, Australia, and 2Department of Medicine (Royal Melbourne Hospital), The University of Melbourne, Parkville, Victoria, Australia. E-mail: bhasker.amatya@mh.org.au
Accepted Apr 9, 2020; Epub ahead of print Apr 9, 2020
A global pandemic has been declared due to the serious public health risk posed by Coronavirus (COVID-19). The WHO declared COVID-19, a new disease, different from other viruses such as Severe Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS) and influenza, as a ‘pandemic’ on 12th March 2020 (1). The number of infected cases with COVID-19 and the human toll is escalating worldwide. Economic losses have skyrocketed and expected to increase in coming months and will exceed capacity of both developing and developed countries. There were more than 777,000 cases, over 37,000 deaths; and 164,446 people recovered worldwide (as of 31 March 2020) (2). The spectrum of disease severity is wide and still evolving. It can range from an asymptomatic infection, mild upper respiratory tract illness to severe viral pneumonia with respiratory failure and death. It is estimated that 80% of cases are asymptomatic or mild; 15% of cases are severe (infection requiring oxygen); and 5% are critical requiring ventilation and life support (3, 4). The mortality rate for COVID-19 is estimated to be 3 to 5% and is higher than for influenza (0.1%) (5). Almost half of all patients admitted to hospital (42%) will require oxygen therapy, with approximate 5% requiring admission to intensive care unit (ICU) (3). The key risk factors for developing severe COVID-19 disease and requiring hospitalisation (and/or ICU support) include: older individuals, male, those with at least one co-existing comorbidity, higher severity of illness scores, elevated d-dimer levels and/or lymphocytopenia (3, 4, 6).
Depending on the severity of COVID-19 impact, patients may suffer a range of functional and psychological impairments during both acute and sub-acute stages, specifically respiratory insufficiency, dyskinesia, neuromuscular and cognitive impairments, and stress etc. Emerging reports from most effected countries like China, South Korea, Italy, Spain, suggest that in addition to more commonly recognized respiratory symptoms, other clinical presentation/complications also relevant to rehabilitation include: posterior revers-ible encephalopathy syndrome, critical illness myopathy/neuropathy following acute respiratory distress syndrome and extracorporeal membrane oxygenation; neuromuscular illness along with plantar flexion contractures and wounds, mental health problems (3, 7–10). Recent data suggests that COVID-19 virus also effects the central nervous system (CNS). COVID-19 related neurological symptoms can be categorized into 3 groups: neurological expressions of the symptoms of the underlying disease (headache, dizziness, disturbances of state of consciousness, ataxia, epileptic manifestations and stroke); symptoms of neuro-peripheral origin (hypo-ageusia, hyposmia, neuralgia); and symptoms of skeletal muscle damage, often associated with liver and kidney damage (9). One recent study in Wuhan, China, reported neurologic manifestations in over one-third of patients (36.4%), with more severe cases likely to have neurologic symptoms such as acute cerebrovascular diseases, impaired consciousness and skeletal muscle injury (8). Similar pattern of neurological syndromes are reported from University of Brescia, Italy (9). The hospital opened an 18-bed neuro-COVID-19 unit (to separate COVID-19 patients from other patients) to treat COVID-19 patients for stroke, delirium, epileptic seizures, and non-specific neurologic syndromes like encephalitis (9). Likewise, other hospitals in Northern Italy are also experiencing dramatic increase in COVID-19-related number of vascular events, ischemic strokes, and thrombosis, likely due to the virus affecting coagulating mechanisms. It is still unclear whether these neurologic syndromes are a direct cause of the virus entering the CNS, or an indirect response to the viral storm in their bodies (9). Further, a wide range of cognitive and psychological disorders have been reported in this patient population. These include: mood alterations (depression), anxiety disorder and suicidal ideas, organic hallucinosis (visual and auditory hallucinations), behavioral disturbances, delusions of persecution, temporal-spatial disorientation, hypomanic disorder, etc. (9, 10). These alarming figures signify the upcoming challenges for the healthcare sectors, specifically rehabilitation both in the short and over the longer term. In the short-term rehabilitation service wards may be occupied by acute COVID-19 patients, due to increased acute care demand. Patients who will survive the COVID-19 will likely need post-acute care to recover from the deficits.
The COVID-19 pandemic has overwhelmed the acute health sector in many countries, especially emergency departments, ICUs, laboratory, radiology services etc. As the situation worsens, it will impact rehabilitation. Although limited data is available to suggest the proportion of COVID-19 patients requiring post-acute care globally. However, historical data from the USA of patients requiring hospitalization following sepsis (a condition with similar inpatient mortality to COVID-19) suggests that approximately 20% required facility-based care and 20% needed care at home (11). With the predicted surge of COVID-19 there will be increasing pressure from acute care to transfer the patients to inpatient rehabilitation facilities (and home rehabilitation, nursing home facilities and other long-term care providers) to free up acute beds. Patients may not be able to be transferred from hospital to these facilites directly given risk of transmitting disease. Currently there are no guidelines as to how long a patient remains contagious following clinical recovery (12). Although rehabilitation in the patient’s own home is an option, this will be limited by inability to manage high acuity patients with COVID-19. Therefore, care models where institutions provide ‘hospital at home’ services are more feasible (13). Delivery of ambulatory care services will need to use ‘Telemedicine’ rather than face-to-face care model, where possible. This will have significant impact on patients and families/carers, and healthcare system at large.
Following the guidance and recommendation from the WHO (5, 14), many Governments worldwide have implemented extensive measures, such as immediate case detection and surveillance, rapid diagnosis and immediate case isolation, rigorous tracking and quarantine of close contacts, and public health prevention measures to reduce the spread of disease. In absence of an effective therapeutic agent or a vaccine, widescale ‘social distancing’ (1.5 m) to limit spread of infection, including local and national lockdowns, banning of mass gatherings and/or public events, personal hygiene (hand washing, regular showers), ‘self-isolation’, are the primary interventions to flatten the escalating epidemiological curve. These effective measures have shown some promising results in countries like China, Korea, Singapore, Australia and others (15, 16). Recent reports from China suggest that after strict case isolation and quarantine, movement restrictions resulted in a downward trend in the number of confirmed new cases (16).
In recent disasters, significant improvements have been achieved in international and regional collaboration, and capacity management, governance, preparedness, and risk-identification. The initiatives by United Nation’s coordinated appeal ‘Global humanitarian response plan COVID-19’ (15) and WHO’s key ‘Strategic Preparedness and response plan for COVID-19’ (14) are much-needed steps for controlling and managing the pandemic worldwide. Further various clinical practice guidelines and protocols are currently being published, with set standards for all healthcare professionals including, rehabilitation personnel to use these minimum standards when responding to current pandemic (4, 15, 17–19).
COVID-19 appears to differ with respect to severity and contamination patterns, with much to learn about the disease and its impact in different contexts. Therefore actions will continue to be driven by rapidly accumulating scientific and public health knowledge (14). Currently, stopping transmission of the virus and reducing mortality is an urgent health priority hence most attention has been on acute management of these patients. Post-acute management and rehabilitation of the current COVID-19 patients and those in recovery is less prioritised. In the coming months, epidemiological modelling predicts that healthcare facilities, specifically sub-acute care, will be overwhelmed by demand as many COVID-19 survivors will require rehabilitative care. Regrettably, subacute care and rehabilitation facilities in many countries currently lack the capacity and capability to safely treat patients with COVID-19, as they transition from hospital to home or to other care settings (20, 21). Regardless, trained skilled staff will be key limiting factor, magnified by this pandemic. Other challenges include availability of personal protective equipment (PPE) and staff COVID-19 testing to ensure they are not transmitting the disease. This is especially challenging in many developing countries where access to rehabilitation, trained staff and PPE is already limited (22).
The WHO defines medical rehabilitation as ‘a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions (disease (acute or chronic), disorder, injury or trauma) in interaction with their environment’ (23). The evidence suggests that during disasters, early involvement of rehabilitation reduces disability, improves clinical outcomes and participation (12, 24). Similar to other disasters, effective rehabilitation in pandemics include: management of the condition (impairments/disabilities), prevent complications, optimize functional capabilities (including cognitive, neuropsychological function), and social re-integration of patients in view of contextual factors that impact functional performance (22, 25). This is especially important as people who survive COVID-19 will require rehabilitation following ICU and/or acute hospital stay, for respiratory and/or neurological impairments, deconditioning and multisystem complications.
Rehabilitation can play an important role in the current pandemic setting. Rehabilitation physicians (and/or allied health/nursing) should be included in the interdisciplinary acute-hospital COVID-19 treating teams. Rehabilitation physicians are not only trained in diagnosis and treatment of general health conditions but are also experts in disability and ‘functioning’. They can coordinate member roles, in the context of patient’ clinical and rehabilitation needs and perform a role in integrating rehabilitation efforts with other health strategies and providers (24). Currently, there is a window of opportunity for authorities and policy makers to integrate the rehabilitation professionals in the midst of the coronavirus pandemic (21, 26). Their potential roles of rehabilitation professionals is to recommend a best practices approach (based on evidence to date), reinforce public health measures- social distancing, self-isolation, hygiene measures; advise/educate patients (and families) about optimizing physical and nutritional health; raise public awareness; assist with communication with primary care physicians, actions and activities to return the patients to a safe environment and successful reintegration into the community.
During this pandemic, the rehabilitation community faces unprecedented challenges due to increased demand for rehabilitative care to COVID-19 patients during their recovery phase. Special consideration will be needed to address safety and care of elderly patients and those with pre-existing comorbidities and disabilities in rehabilitation facilities (6). Rehabilitation professionals will provide disability management and assessment in the context of evolving disease pattern, changing clinical needs, treatment and management of the condition and complications, and longitudinal follow-up. The potential challenges include:
Integrating rehabilitation personnel in acute-care COVID-19 clinical teams, provide patient assessment whilst in acute setting for range of disabilities in the recovery phase.
Provide safe physical environments within rehabilitation wards that comply with social distancing and hygiene, allocated ward spaces for COVID-19 and non-COVID patients and their treating clinical and non-clinical teams, etc.
Mitigate risk (as able) for a potential COVID-19 exposure to patients and staff- comply with COVID-19 Guidelines, limit visitor numbers, screening of staff and visitors for temperature and hand hygiene, etc.
Allocation health care resources in rehabilitation facilities (trained workforce, PPE, equipment, infrastructure).
Manage psychological distress in staff and patients by identifying at risk people and appropriate timely intervention.
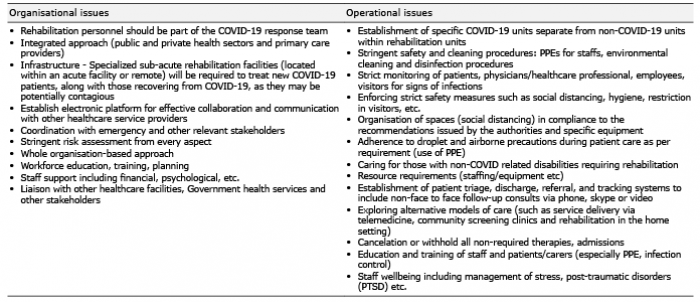
The rehabilitation needs and demand for COVID-19 survivors can vary in various settings and over time, however, rehabilitation is essential in all phases of pandemic management. There is a need for an integrated system to enhance capacities of healthcare institutions in the prevention and management process of this pandemic. Some potential recommendations for rehabilitation approach of the COVID-19 patients is detailed in Table I below (4, 7, 19, 21).
Table I. Potential recommendations for rehabilitation approach of the COVID-19 patients
In conclusion, the novel COVID-19 is having a devastating effect worldwide, and the situation is still evolving. The control of spread of disease and management of these patients is a daunting challenge in modern times. Prevention, response management plans and standards will continue to be driven by rapidly accumulating scientific and public health knowledge. As in any disaster, the role of medical rehabilitation in pandemics is an integral component of comprehensive management. Early rehabilitation of the COVID-19 patients can enhance pulmonary, respiratory function, reduce complications, improve function, cognitive impairments and quality of life (8–10, 12, 27).
There is need for a coordinated, collaborative approach for managing COVID-19 with relevant national and international organisations and stakeholders for acute response, rehabilitation and recovery. The WHO, and International Society of Physical and Rehabilitation Medicine (ISPRM) are key players to facilitate coordination amongst 77 National Societies of Physical Medicine and Rehabilitation globally to assist with action needed in this pandemic. However, effective rehabilitation-inclusive pandemic response and management will depend on the capacity and willingness of countries to learn from shared experiences and build a systematic advance planning and preparedness to ensure that effective services are available to those who need it.
We acknowledge the Disaster Rehabilitation Committees (DRC), of the International Society of Physical and Rehabilitation Medicine (ISPRM) and Disaster Rehabilitation Special Interest Group, of the Rehabilitation Medicine Society of Australia and New Zealand (RMSANZ) for their support. The views express in this article are not of the above-mentioned committees.
The authors have no conflicts of interests to declare.


 Click to show fullsize
Click to show fullsize